
Catamenial pneumothorax (CPT) differs from Spontaneous pneumothorax (SPT)
SPT vs. CPT
Spontaneous pneumothorax (SPT) is a well known condition among physicians. Air enters the pleural space around the lung, and causes the lung to collapse (1). What makes it spontaneous is that the collapse can occur without warning in a person who appears healthy. As Lynn's Pulmonary Specialist described it, "the lung collapses for no apparent reason." Medically, this may be due to the rupture of "blebs", which are blister-like appendages on the lung. Blebs and bullae are generally confirmed through surgery (1).
SPT primarily affects tall thin men in their 20's and 30's (1). Women can also experience SPT, but statistically it is rare. As such, it is not unreasonable to speculate that some women diagnosed with or treated for spontaneous pneumothorax, may actually have catamenial pneumothorax (CPT or CP), which is not spontaneous at all! This is especially true for women who have had multiple collapses.
CPT
Catamenial pneumothorax is a rare condition characterized by a re-occurrence of air in the pleural space coinciding with the onset of menses (2). This condition was first described in literature in 1958 (3). It is almost always right-sided, and generally affects women in their 30's and 40's (4, 5).
Although the exact etiology of the condition is unknown, most physicians agree that endometriosis is involved (4). In the literature, this condition is described as thoracic endometriosis (TE), thoracic endometriosis syndrome (TES), or thoracic endometriosis-related pneumothorax (TERP). Documented case studies have described endometrial implants on the lung or pleura (6). More frequently however, articles describe cases involving diaphragmatic fenestrations (holes in the diaphragm) (1). Some researchers attribute this damage to endometriosis and speculate that air passes into the pleural space through these holes (4, 6, 10). Endometriosis is also thought responsible for corresponding hemothorax (blood in the pleural space) as well as hemoptysis and intra-thoracic endometrial nodules (7).
Case studies report that women with CPT experience monthly chest pain, shortness of breath, dizziness and fatigue. Some women have experienced multiple lung collapses over a period of several years. Many of these women have also been diagnosed with pelvic endometriosis (5).
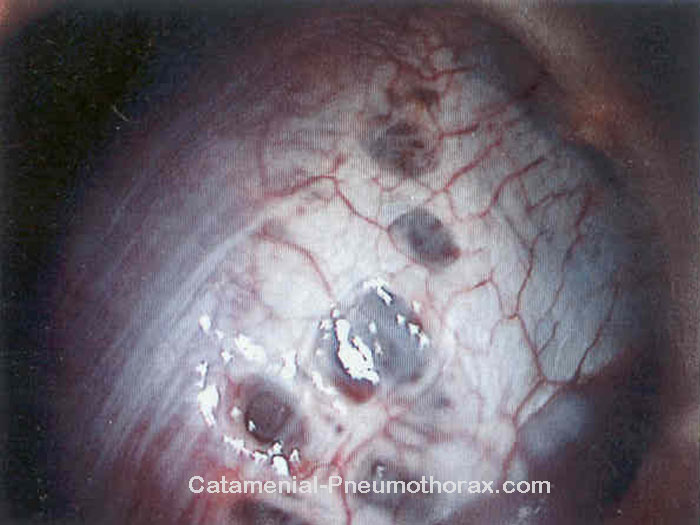
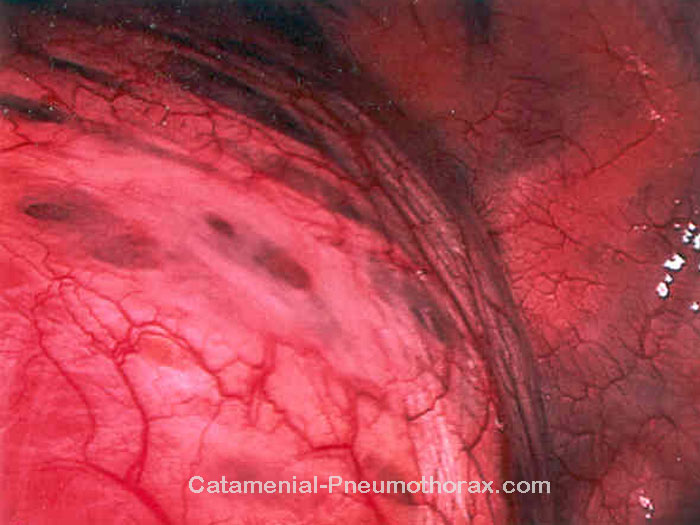
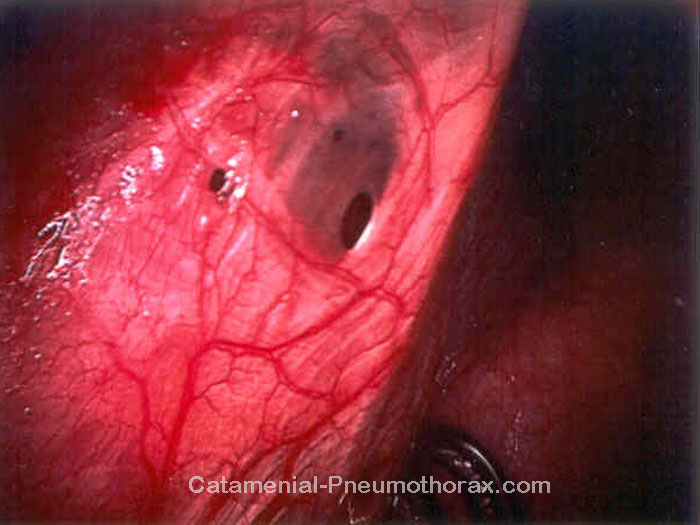
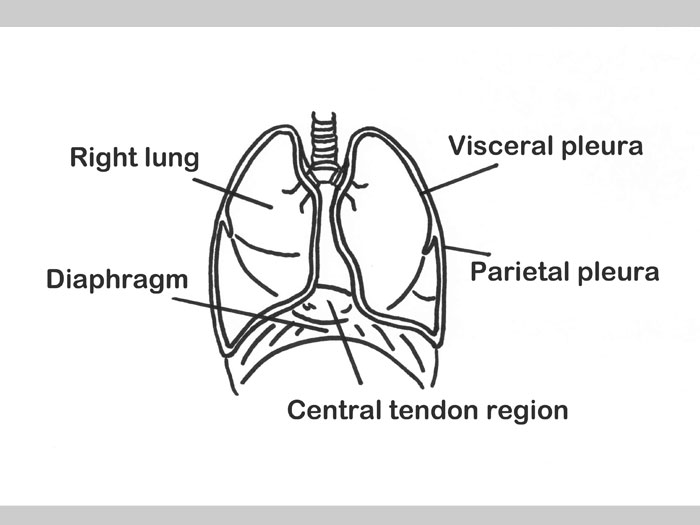
Images
One benefit of video-assisted thoracic surgery (VATS) is that images can be captured during the procedure. Treatment of catamenial pneumothorax often involves diaphragm repair in order to close up the fenestrations (8). Due to their appearance, the holes are sometimes described as resembling "blueberry spots" (9). The first two images are from Lori's surgery, where the blueberry effect can readily be seen. The next three images are from Lynn's surgery, which show diaphragmatic fenestrations as well as scarred pleura. Fenestrations are generally found on the central tendon region of the diaphragm (9) as shown in the illustration.


CPT Fact Sheet - A Summary for your Doctor
When we first developed the web site, we learned that several women were printing the pages to take to their doctors, with the hope that the information would assist them in getting a definitive diagnosis of catamenial pneumothorax.
Knowing that doctors are busy people and unlikely to read multiple internet pages brought in by their patients, we prepared a two-page printer-friendly fact sheet, which provides an overview and summary of CPT in a pdf file. It contains important definitions, symptoms of the condition, treatment options, images of diaphragmatic fenestrations, and literature references.
Clicking on the image will open the file, allowing you to print and/or save the document.
Useful Links and References
Pneumothorax.org (Information on spontaneous pneumothorax)
Geneva Foundation for Medical Education and Research (Additional images of CPT)

(1) Guidelines for the diagnosis and treatment of spontaneous pneumothorax. Rivas de Andres JJ, Jimenez Lopez MF, Lopez-Rodo LM, Perez Trullen A, Torres Lanzas J. J Arch Bronconeumol. 2008;44(8):437-48
(2) Thoracic endometriosis: current knowledge. Alifano M, Trisolini R, Cancellieri A, Regnard JF. Ann Thorac Surg. 2006 Feb;81(2):761-9
(3) Chronic recurring spontaneous pneumothorax due to endometriosis of the diaphragm. Maurer ER, Schaal JA, Mendez FL. JAMA. 1958;168:2013-2014
(4) Catamenial pneumothorax: retrospective study of surgical treatment. Bagan P, Barthes FL, Assouad J, Souilamas R, Riquet M. Ann Thorac Surg. 2003 Feb;75(2):378-381
(5) Recurrent spontaneous pneumothorax associated with menstrual cycle: report of three cases of catamenial pneumothorax. Choong CK, Smith MD, Haydock DA. ANZ J Surg. 2002 Sep;72(9):678-679
(6) Catamenial pneumothorax caused by thoracic endometriosis. Van Schil PE, Vercauteren SR, Vermeire PA, Nackaerts YH, Van Marck EA. Ann Thorac Surg. 1996 Aug;62(2):585-586
(7) Management of thoracic endometriosis: single institution experience. Duyos I, Lopez-Carrasco A, Hernandez A, Zapardiel I, de Santiago J. Eur J Obstet Gynecol Reprod Biol. 2014 Jul;178:56-59
(8) Diaphragmatic fenestrations in catamenial pneumothorax: a management strategy. Rafay M, El-Bawab H, Kurdi W, Al Kattan K. Asian Cardiovasc Thorac Ann. 2009 Jan;17(1):70-72
(9) Catamenial pneumothorax due to diaphragmatic endometriosis confirmed by histological examination: report of a case. Segawa M, Touge M, Kusajima Y, Saito K. Kyobu Geka. 2011 May;64(5):430-433
(10) Catamenial pneumothorax associated with multiple diaphragmatic perforations and pneumoperitoneum in a reproductive woman. Baoquan L, Liangjian Z, Qiang W, Hai J, Hezhong C, Zhiyun X. J Formos Med Assoc. 2014 Jun;113(6):385-387